
COVID-19 Cases, Hospitalizations, and Deaths: Can the Official Numbers be Believed?
COVID-19 Cases, Hospitalizations, and Deaths: Can the Official Numbers be Believed?

Originally published on Medium 4 May 2021
The coronavirus pandemic has served as justification for restrictions on human liberty unparalleled in the peacetime history of any nation any time in the last century. These restrictions have exacted a toll including but not limited to joblessness, rent delinquency, homelessness, depression, substance abuse, suicidality, and skyrocketing rates of death due to “unintentional injury.”
But all this was justified, we were told, as the news anchors warned us night after night of the mounting toll of cases, hospitalizations, and deaths due to the covid. As the pandemic continues into its second year, this seems like a good time to take a look at just how reliable these figures are.
Can the PCR Test Results Be Believed?
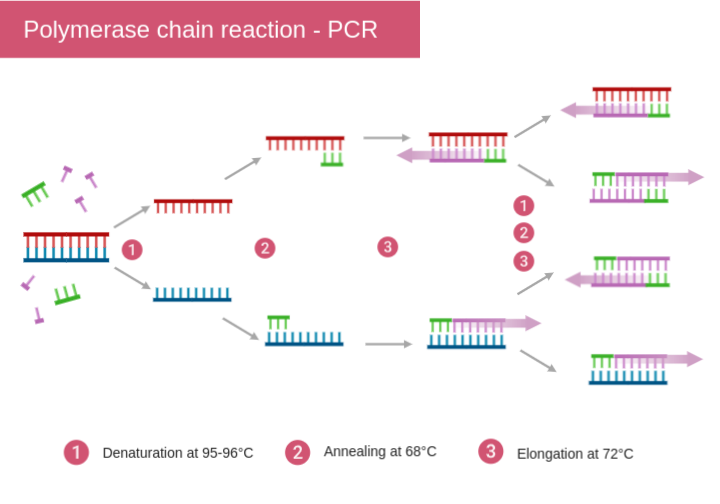
The figures for COVID-19 cases, hospitalizations, and deaths are based in a large measure on the quantitative PCR Test for viral genetic material. PCR stands for Polymerase Chain Reaction, a process for making a large amount of DNA from a small one. This process was invented by the biochemist Kary Mullis, a feat which earned him the 1993 Nobel Prize in Chemistry.
In the polymerase chain reaction, first the DNA of interest is placed in a test tube along with nucleotides and heat-resistant DNA polymerase derived from Thermus aquaticus, a bacterium normally found at near-boiling temperatures in hot springs and hydrothermal vents. When the mixture is cooled, the DNA polymerase does its work, synthesizing a complementary strand for each of the single strands of DNA and so, lo and behold, you now have two copies of the original DNA helix. Repeat the cycle of heating and cooling, and now you have four copies. Repeat again and you have eight. Each cycle of heating and cooling doubles the original amount of DNA. Forty cycles of heating and cooling will increase the initial amount of DNA by a factor of two multiplied by itself forty times, or a little over one trillion, and so a tiny soupçon of DNA can be amplified into a very large amount in a very short period of time.
The number of cycles of heating and cooling needed to produce a measurable amount of DNA is called the Cycle threshold (Ct). The smaller the initial amount of DNA, the higher the cycle threshold needed to detect it will be. This is an important point.
Why? Because the fact that a small amount of viral genetic material can be found does not necessarily mean a given patient is infected with the virus, or is capable of transmitting the infection to others. It may simply be indictive of a small amount of viral genetic material that was left over after the body had already conquered the infection, or for that matter was just floating around in the environment at the time the sample was taken. The only way to verify a given patient is infected is to take a sample of that patient’s body fluids, use it to inoculate cells in culture dishes, and recover intact virus particle from those cells.
A French study of 183 samples found that those with Cycle threshold values between thirteen and seventeen all were capable of producing replication-competent virus. As Ct values exceeded seventeen, infectivity dropped sharply. No samples with Ct values above thirty-three could produce replication-competent virus.
Another more comprehensive study of 3,790 samples by the same research team corroborated these results, finding that less than three percent of sample with Ct values of thirty-five or greater were infectious.
The CDC and the FDA do not specify a specific Cycle threshold for a diagnosis of COVID-19, but an article in the New York Times reported that most testing companies set that threshold at forty cycles — a value guaranteed to ensure false positive results.
It Gets Awkward
There are other ways by which the official numbers of cases, hospitalizations, and deaths may have been inflated. Official CDC guidelines, drawn up by the Council of State and Territorial Epidemiologists, do not require PCR or any specific laboratory test for a case of COVID-19 to be added to the official numbers. Two symptoms from a checklist of ten, or one symptom from a checklist of five, is enough. These symptoms (fever, chills, headache, etc.) could be the symptoms of any number of other conditions, but no matter. A simple cough can be enough for a diagnosis of COVID-19 to be rendered — provided that, in the diagnostician’s judgement, no other diagnosis is more likely.
In regard to deaths, only five percent of those said to have died from the coronavirus had COVID-19 listed as the sole cause on the death certificate. The remaining ninety-five percent had an average of FOUR causes or comorbidities each, including influenza, chronic lower respiratory disease, hypertensive disease, ischemic heart disease, cerebrovascular disease, sepsis, malignant neoplasm, diabetes, obesity… The list goes on and on.
So how to decide whether the coronavirus was the actually the cause of a given patient’s death or just came along for the ride? The law provides diagnosticians and hospitals with a powerful incentive to classify as many hospitalizations and deaths as possible as due to the coronavirus, by means of the Coronavirus Aid, Relief, and Economic Security (CARES) Act, which provides extra reimbursement for COVID-19 cases.
Scott Jensen, a medical doctor and former state senator in Minnesota told Fox News:
Any time health care intersects with dollars, it gets awkward. Right now, if you have a COVID-19 admission to the hospital, you’ll get paid thirteen thousand dollars. If that COVID-19 patient goes on a ventilator, you’ll get thirty-nine thousand dollars — three times as much. Nobody can tell me, after thirty-five years in the world of medicine, that sometimes those kinds of things impact on what we do.
Public health officials are charged with making decisions that impact the life and death of millions of people ought to base their decisions on data that is as accurate and unbiased as possible. That doesn’t seem to be what is going on here.
Conspiracy Theories
The same Fox News segment offered these words of wisdom from NIAID Director Anthony Fauci:
You will always have conspiracy theories when you have very challenging public health crises. They are nothing but distractions.
That may be. But as anyone who has ever dealt with a hospital billing department already knows, when all the mistakes are in their favor, you have to wonder.
So where does this leave us? According to the CDC, as of 3 October 2020, the United States had racked up 300,000 excess deaths, with 200,000 of these attributed to the covid and the remaining 100,000 to other causes. So already they have conceded that excess deaths due to other causes are on a scale comparable to that of covid deaths.
Moreover, we have already seen the system is biased toward over-reporting covid deaths. What if just twenty-five percent of putative covid deaths were not, in fact, due to the covid? That would mean the number of excess deaths due to other causes would be equal to the number of excess deaths due to the covid.
In the absence of any convincing argument to the contrary, we probably ought to assume that the excess deaths due to “other causes” were in fact indirect effects of the covid restrictions. We know that deaths due to “unintentional injuries” have soared during the pandemic. How many of these were people driven to rage or despair by the disruption the covid restrictions have wrought upon their lives? Excess deaths due to heart disease, Alzheimer’s, and diabetes have also soared. How many of these were elderly folks who died of loneliness and despair after being deprived of the one thing that could bring meaning to their final days on earth — the opportunity to share their love and wisdom with friends and family?
It could easily be that the number of excess deaths due to the covid restrictions was equal to the number caused by the virus itself. And the picture could be even more dismal if we analyzed these data in terms of number of years of life lost. It may be that the average age of excess deaths due to other causes such as unintentional injuries was lower than that those due to the covid. If this be the case — and admittedly this is speculative — that would mean we have crossed the line over from mismanagement of a crisis to state-sponsored mass homicide.
Again, admittedly this is speculative. But it may be significant that nobody who is in a position to perform the definitive analysis seems interested in doing so.
wow, late to the party on this AWESOME article. I just posted an article with a PCR test deep dive.